TMJ Guide
Tennis Elbow vs Golfer's Elbow: Key Differences (2026)
Tennis elbow vs golfer's elbow: learn the key differences in pain location, tendons, symptoms, and treatment. Expert sports medicine guide to identifying your condition.
By Dr. Michael Torres · Published 2026-03-21 · Updated 2026-03-21
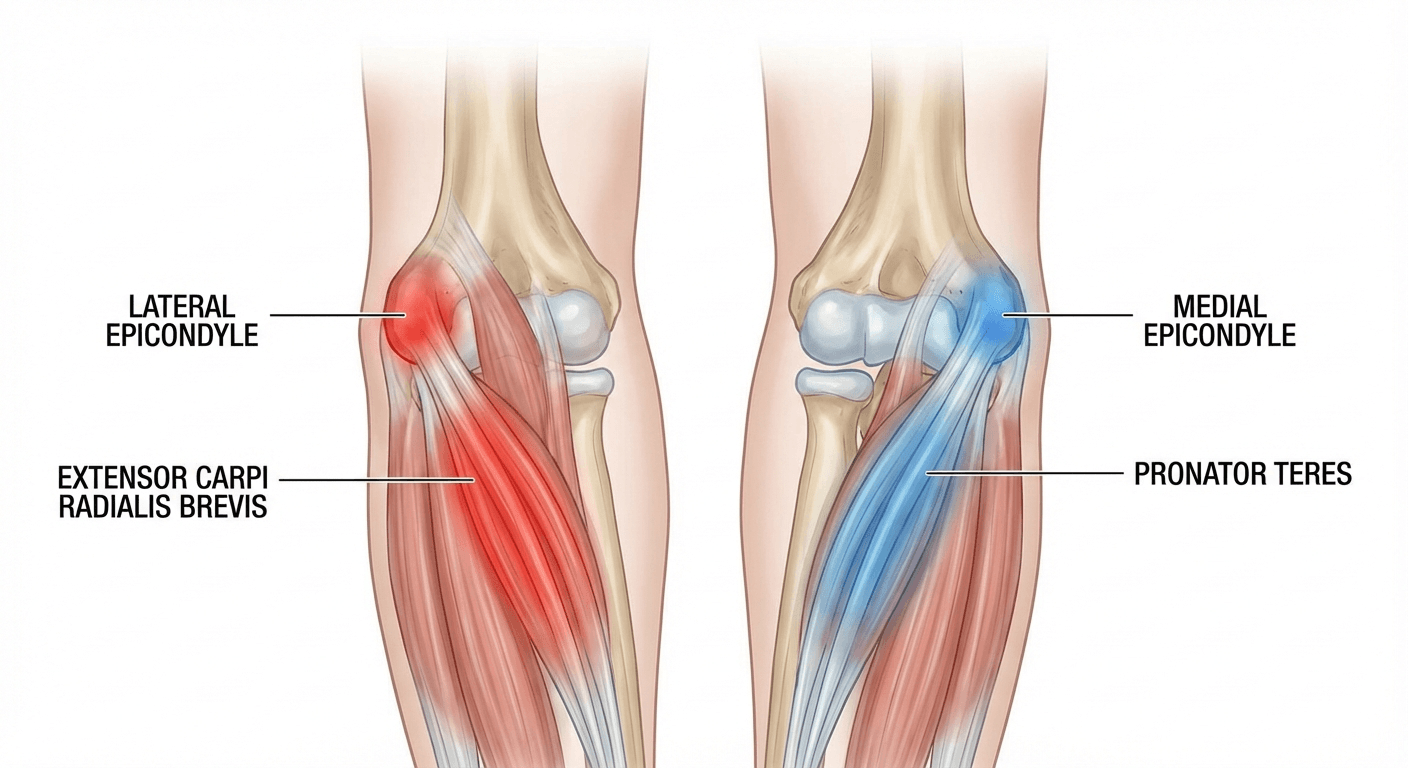
Tennis elbow (lateral epicondylitis) affects the outside of the elbow, while golfer's elbow (medial epicondylitis) affects the inside. Both are overuse injuries caused by repetitive forearm motions, but they involve different tendons, trigger different pain patterns, and often respond to slightly different treatment approaches. Understanding which condition you have is essential for effective recovery.
By Dr. Michael Torres, Sports Medicine & Rehabilitation Specialist Last updated: March 2026
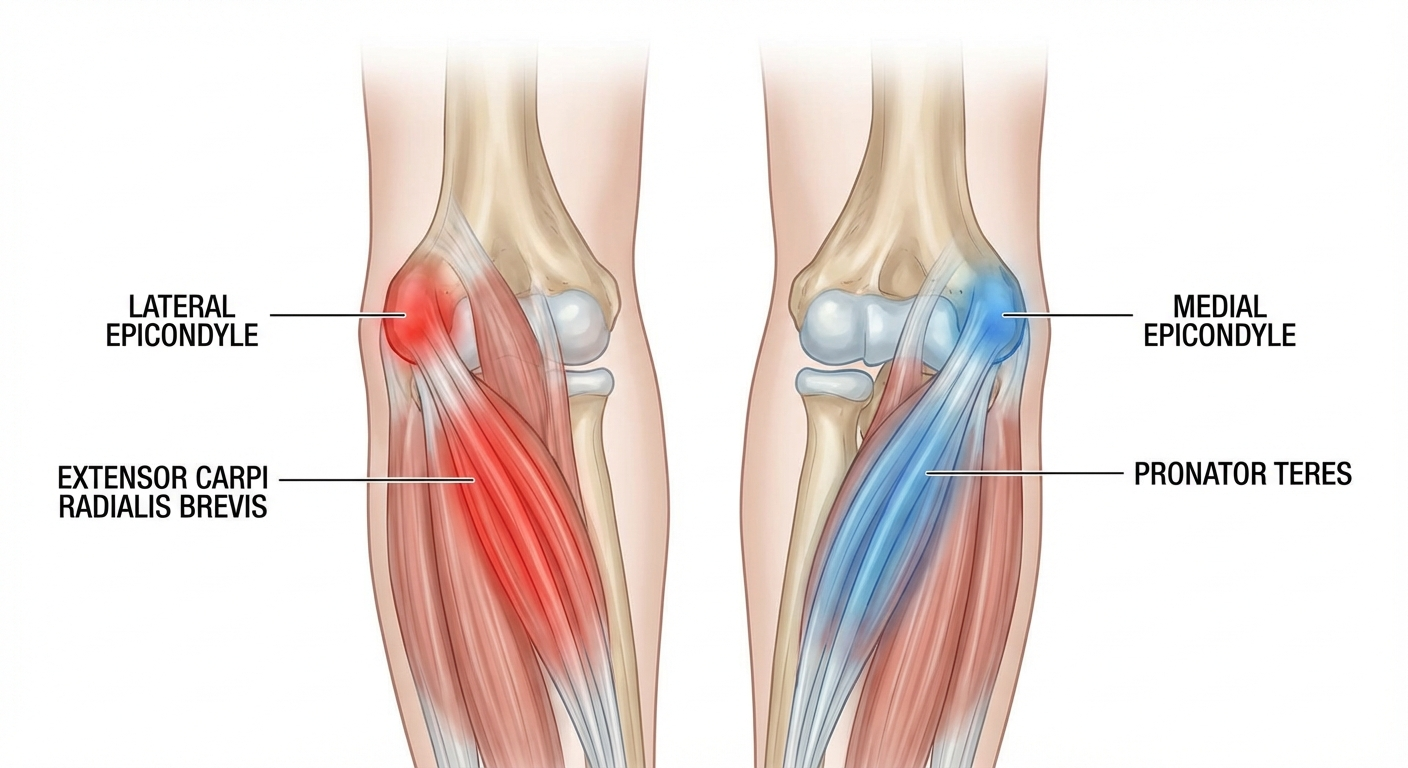 The key difference: tennis elbow hurts on the outside of your elbow; golfer's elbow hurts on the inside.
The key difference: tennis elbow hurts on the outside of your elbow; golfer's elbow hurts on the inside.
Table of Contents
- What Is Tennis Elbow?
- What Is Golfer's Elbow?
- Tennis Elbow vs Golfer's Elbow: Side-by-Side Comparison
- Anatomy: Why the Location Matters
- Causes and Risk Factors
- Symptoms: How to Tell Them Apart
- Diagnosis
- Treatment Options
- Which Heals Faster?
- Can You Have Both at the Same Time?
- Prevention Strategies
- When to See a Doctor
- Frequently Asked Questions
- Sources
What Is Tennis Elbow?
Tennis elbow, clinically known as lateral epicondylitis, is a painful condition that develops when the tendons on the outer (lateral) side of your elbow become overloaded. Despite its name, tennis elbow is not exclusive to tennis players. In fact, studies suggest that fewer than 10% of people diagnosed with lateral epicondylitis actually play tennis. The condition is far more common among plumbers, painters, carpenters, butchers, and office workers who spend long hours using a mouse and keyboard.
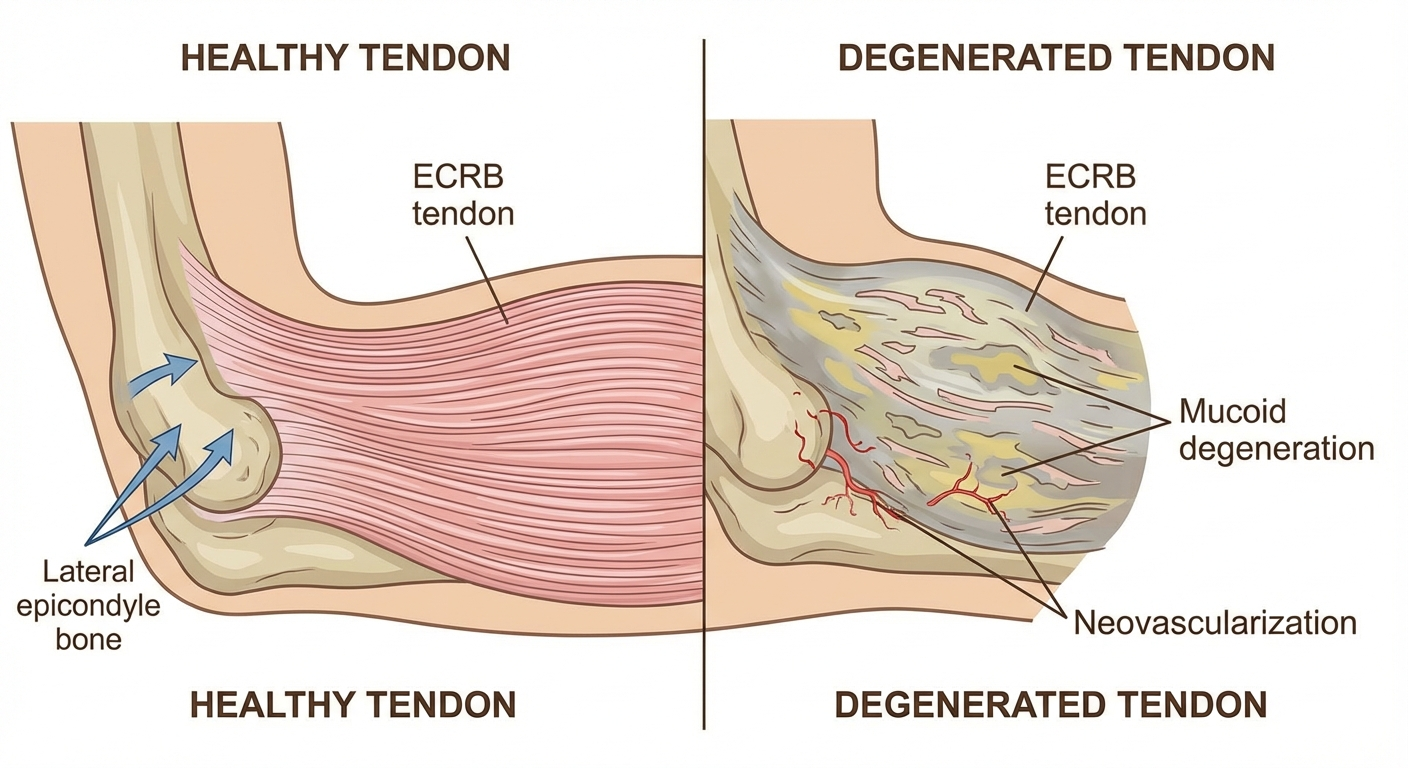
The primary tendon involved is the extensor carpi radialis brevis (ECRB), which helps stabilize the wrist when the elbow is straight. When you repeatedly grip, twist, or extend your wrist, microscopic tears develop in this tendon where it attaches to the lateral epicondyle — the bony bump on the outside of your elbow. Over time, these micro-tears accumulate faster than the body can repair them, leading to a cycle of degeneration rather than true inflammation.
Modern research has shifted our understanding of tennis elbow from an inflammatory condition ("-itis") to a degenerative one. Histological studies consistently show disorganized collagen fibers and an absence of inflammatory cells in chronic cases. This is why the condition is sometimes more accurately called lateral epicondylalgia or lateral epicondylar tendinopathy.
Tennis elbow affects approximately 1-3% of the general population, with a peak incidence between ages 35 and 54. It is equally common in men and women and typically affects the dominant arm.
 Unlike true inflammation, tendinopathy involves degenerative collagen changes — this is why anti-inflammatories have limited long-term effectiveness.
Unlike true inflammation, tendinopathy involves degenerative collagen changes — this is why anti-inflammatories have limited long-term effectiveness.
What Is Golfer's Elbow?
Golfer's elbow, or medial epicondylitis, is the counterpart condition affecting the inside (medial) side of the elbow. It involves the tendons of the forearm flexor muscles — specifically the pronator teres and the flexor carpi radialis — where they attach to the medial epicondyle.
Like tennis elbow, golfer's elbow is poorly named. While it does occur in golfers (particularly those with flawed swing mechanics), it is far more common in people who perform repetitive gripping, throwing, or wrist-flexion activities. Rock climbers, weightlifters, baseball pitchers, and workers who use vibrating tools are all at elevated risk.
Golfer's elbow is roughly 3 to 10 times less common than tennis elbow, accounting for roughly 10-20% of all epicondylitis diagnoses. However, it can be just as debilitating. The medial side of the elbow is also home to the ulnar nerve — the "funny bone" nerve — which means golfer's elbow can sometimes produce tingling or numbness radiating into the ring and little fingers.
The underlying pathology mirrors that of tennis elbow: angiofibroblastic degeneration of the tendon rather than acute inflammation. This distinction matters because it influences treatment strategies, particularly the limited role of anti-inflammatory medications in chronic cases.
Tennis Elbow vs Golfer's Elbow: Side-by-Side Comparison
Understanding the differences between tennis elbow and golfer's elbow is easiest when you see them compared directly. The following table breaks down the key distinctions:
| Feature | Tennis Elbow (Lateral Epicondylitis) | Golfer's Elbow (Medial Epicondylitis) |
|---|---|---|
| Pain Location | Outside of the elbow | Inside of the elbow |
| Tendons Involved | Wrist extensors (ECRB) | Wrist flexors (pronator teres, FCR) |
| Painful Movements | Gripping, lifting with palm down, backhand | Gripping, lifting with palm up, throwing |
| Common Activities | Typing, painting, using a screwdriver, tennis backhand | Golf swing, throwing sports, rock climbing, weightlifting |
| Prevalence | 1-3% of population | 0.3-0.6% of population |
| Nerve Involvement | Rare (posterior interosseous nerve) | More common (ulnar nerve — tingling in ring/little finger) |
| Age of Onset | 35-54 years | 35-54 years |
| Dominant Arm | Usually affected | Usually affected |
| Recovery Time | 6-24 months | 6-24 months |
| Surgical Rate | ~5-10% of cases | ~3-5% of cases |
Watch: Tennis Elbow vs Golfer's Elbow Explained
Anatomy: Why the Location Matters
To truly understand the difference between tennis elbow and golfer's elbow, you need a basic grasp of elbow anatomy.
The elbow joint is formed by three bones: the humerus (upper arm bone), the radius, and the ulna (the two forearm bones). At the bottom of the humerus, two bony prominences flare out on either side — these are the epicondyles.
The Lateral Epicondyle (Tennis Elbow Side)
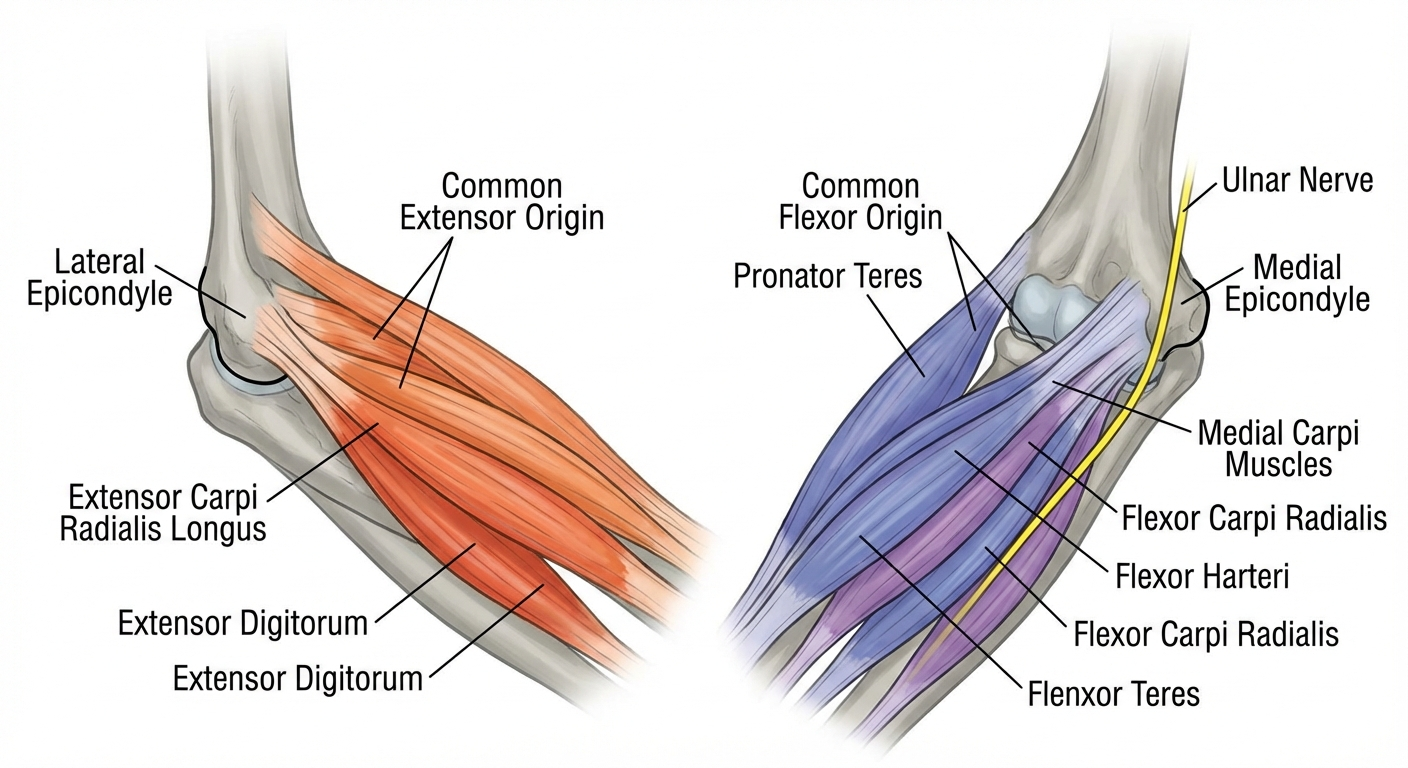
The lateral epicondyle sits on the outer side of the elbow. It serves as the anchor point for the common extensor tendon, a shared tendon through which several forearm muscles attach. These muscles are responsible for extending (straightening) the wrist and fingers. When you perform a backhand stroke in tennis, turn a screwdriver, or type at a keyboard, these extensor muscles do the heavy lifting.
The ECRB tendon, which is the most commonly affected in tennis elbow, has a particularly vulnerable position. It rubs against the lateral epicondyle as the elbow bends and straightens, creating friction that contributes to tendon breakdown over time.
The Medial Epicondyle (Golfer's Elbow Side)
The medial epicondyle sits on the inner side of the elbow. It anchors the common flexor tendon, through which the forearm flexor muscles attach. These muscles control wrist flexion (bending the wrist toward the palm) and forearm pronation (rotating the palm downward). A golf swing, a baseball pitch, or a heavy deadlift all rely heavily on these muscles.
Critically, the ulnar nerve runs through a groove (the cubital tunnel) just behind the medial epicondyle. This anatomical proximity means that medial epicondylitis can irritate or compress the ulnar nerve, producing neurological symptoms that tennis elbow rarely causes. If you are experiencing numbness or tingling in your fingers alongside elbow pain, this is an important diagnostic clue pointing toward golfer's elbow — and potentially ulnar nerve involvement that warrants separate evaluation.
 Color-coded muscle map: orange-red = extensor group (tennis elbow), blue-purple = flexor group (golfer's elbow), yellow = ulnar nerve.
Color-coded muscle map: orange-red = extensor group (tennis elbow), blue-purple = flexor group (golfer's elbow), yellow = ulnar nerve.
Causes and Risk Factors
If your elbow pain is accompanied by wrist symptoms, you may be dealing with multiple repetitive strain injuries simultaneously. CarpaltunnelGuide.com explains the overlap between elbow and wrist RSI and how to address both conditions without aggravating either.
While both conditions stem from overuse, the specific activities that trigger each are quite different.
Tennis Elbow Triggers
- Racquet sports: Particularly the backhand stroke with poor technique or a racquet that is too heavy
- Computer work: Prolonged mouse use and typing, especially with poor ergonomic setup
- Manual trades: Painting, plumbing, carpentry, bricklaying — any repetitive gripping and twisting
- Music: Playing instruments that require sustained wrist extension (e.g., violin, guitar)
- Cooking: Repeated chopping, stirring, and wringing motions
If you are already dealing with tennis elbow from any of these activities, learning the right tennis elbow exercises can be a critical part of your recovery plan.
Golfer's Elbow Triggers
- Golf: Particularly hitting "fat" shots (striking the ground before the ball) or having a death-grip on the club
- Throwing sports: Baseball, javelin, football — the valgus stress during throwing loads the medial tendons
- Weightlifting: Deadlifts, pull-ups, rows, and heavy curls with excessive wrist flexion
- Rock climbing: Sustained gripping on crimps and small holds
- Occupational: Using vibrating tools (chainsaws, jackhammers), assembly line work with repetitive gripping
Shared Risk Factors
Several risk factors increase your likelihood of developing either condition:
- Age: Peak incidence between 35 and 54
- Obesity: BMI above 30 is associated with higher rates of both conditions
- Smoking: Impairs tendon blood supply and healing capacity
- Diabetes: Associated with tendinopathy through glycation of collagen fibers
- Sudden increases in activity: Ramping up training volume or starting a new physical job without gradual adaptation
- Poor biomechanics: Incorrect technique in sport or work tasks places disproportionate stress on tendons
Symptoms: How to Tell Them Apart
The single most reliable way to distinguish between tennis elbow and golfer's elbow at home is pain location.
Tennis Elbow Symptoms
- Pain and tenderness on the outer (lateral) side of the elbow
- Pain worsens when gripping objects, especially with the arm extended
- Weak grip strength, particularly when shaking hands or turning a door handle
- Pain when extending (straightening) the wrist against resistance
- Stiffness in the elbow, especially in the morning
- Pain that radiates down the outer forearm toward the wrist
Golfer's Elbow Symptoms
- Pain and tenderness on the inner (medial) side of the elbow
- Pain worsens with wrist flexion (bending the wrist toward the palm) against resistance
- Weak grip strength when carrying bags or squeezing objects
- Pain during throwing or swinging motions
- Stiffness in the elbow with difficulty making a fist
- Tingling or numbness in the ring and little fingers (if the ulnar nerve is involved)
- Pain that radiates down the inner forearm toward the wrist
A Simple Self-Test
Try these two quick tests at home (stop immediately if you experience severe pain):
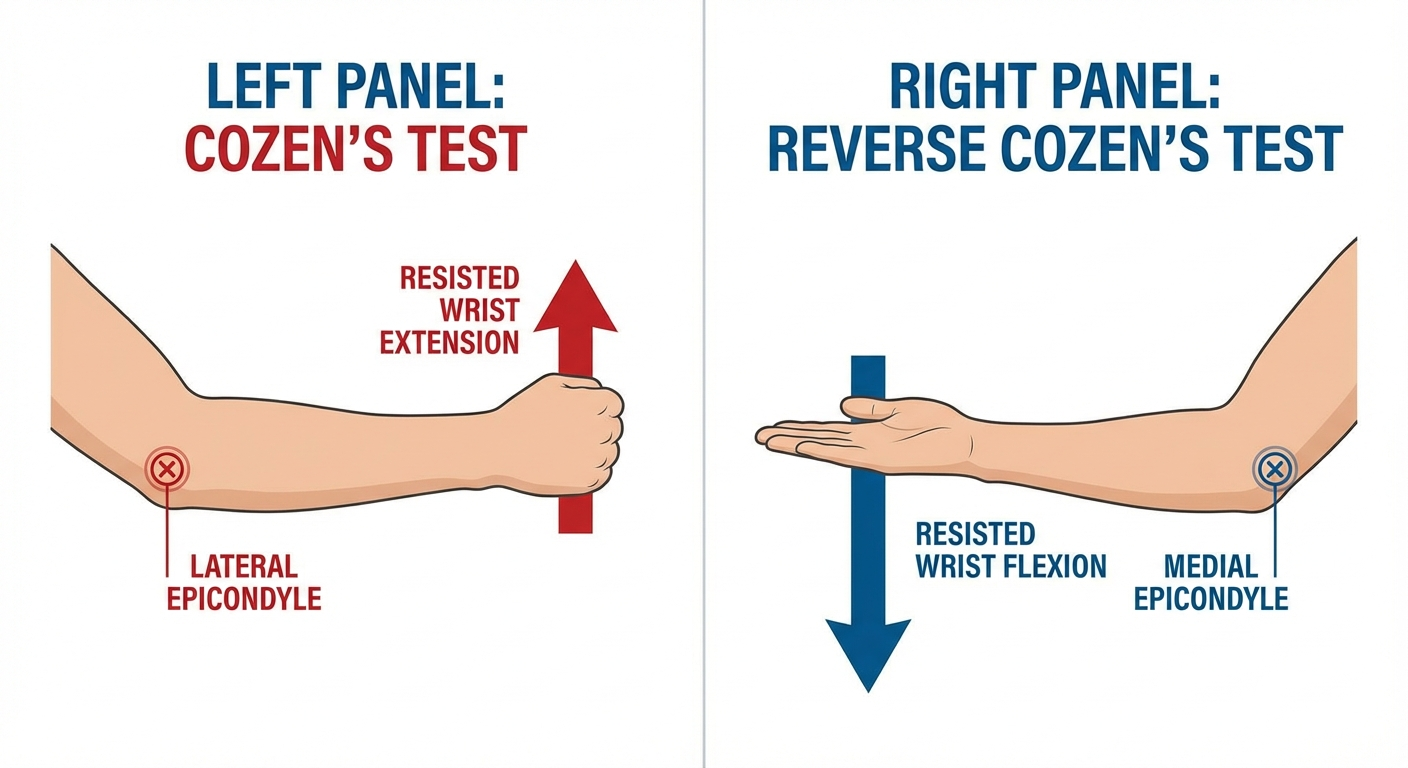
-
Cozen's Test (for tennis elbow): Extend your arm in front of you with your palm facing down. Make a fist and try to extend (raise) your wrist upward while someone pushes it down. If this reproduces pain on the outside of the elbow, tennis elbow is likely.
-
Reverse Cozen's Test (for golfer's elbow): Extend your arm with your palm facing up. Try to flex (curl) your wrist upward while someone pushes it down. If this reproduces pain on the inside of the elbow, golfer's elbow is likely.
 You can perform these self-tests at home, but a physiotherapist diagnosis is always recommended for accurate identification.
You can perform these self-tests at home, but a physiotherapist diagnosis is always recommended for accurate identification.
Diagnosis
While self-assessment can guide you, a proper diagnosis from a qualified healthcare provider ensures you receive the right treatment. Misdiagnosis can lead to months of wasted effort on the wrong rehabilitation program.
Clinical Examination
A sports medicine physician, orthopedic specialist, or physiotherapist will typically perform:
- Palpation: Pressing directly on the lateral and medial epicondyles to locate the exact point of maximum tenderness
- Resisted wrist extension and flexion tests: Isolating the extensor and flexor muscle groups
- Mill's test: Passive stretch of the extensor tendons with the wrist flexed and elbow extended
- Grip strength measurement: Often reduced on the affected side, quantified with a dynamometer
- Neurological assessment: Checking for ulnar nerve involvement (Tinel's sign at the elbow, sensation in the hand)
Imaging
In most cases, imaging is not required for a straightforward diagnosis. However, your doctor may order:
- X-rays: To rule out fractures, arthritis, or calcification within the tendons
- Ultrasound: Highly effective at showing tendon thickening, tears, and neovascularization. Dynamic ultrasound can also assess tendon function during movement
- MRI: Reserved for cases that do not respond to treatment, suspected complete tears, or when surgery is being considered. MRI provides detailed soft tissue visualization and can identify bone marrow edema
Understanding your diagnosis is the first step. The next is knowing how long tennis elbow lasts so you can set realistic expectations for your recovery timeline.
 Both conditions respond best to progressive eccentric loading exercises — passive treatments alone rarely provide lasting relief.
Both conditions respond best to progressive eccentric loading exercises — passive treatments alone rarely provide lasting relief.
Treatment Options
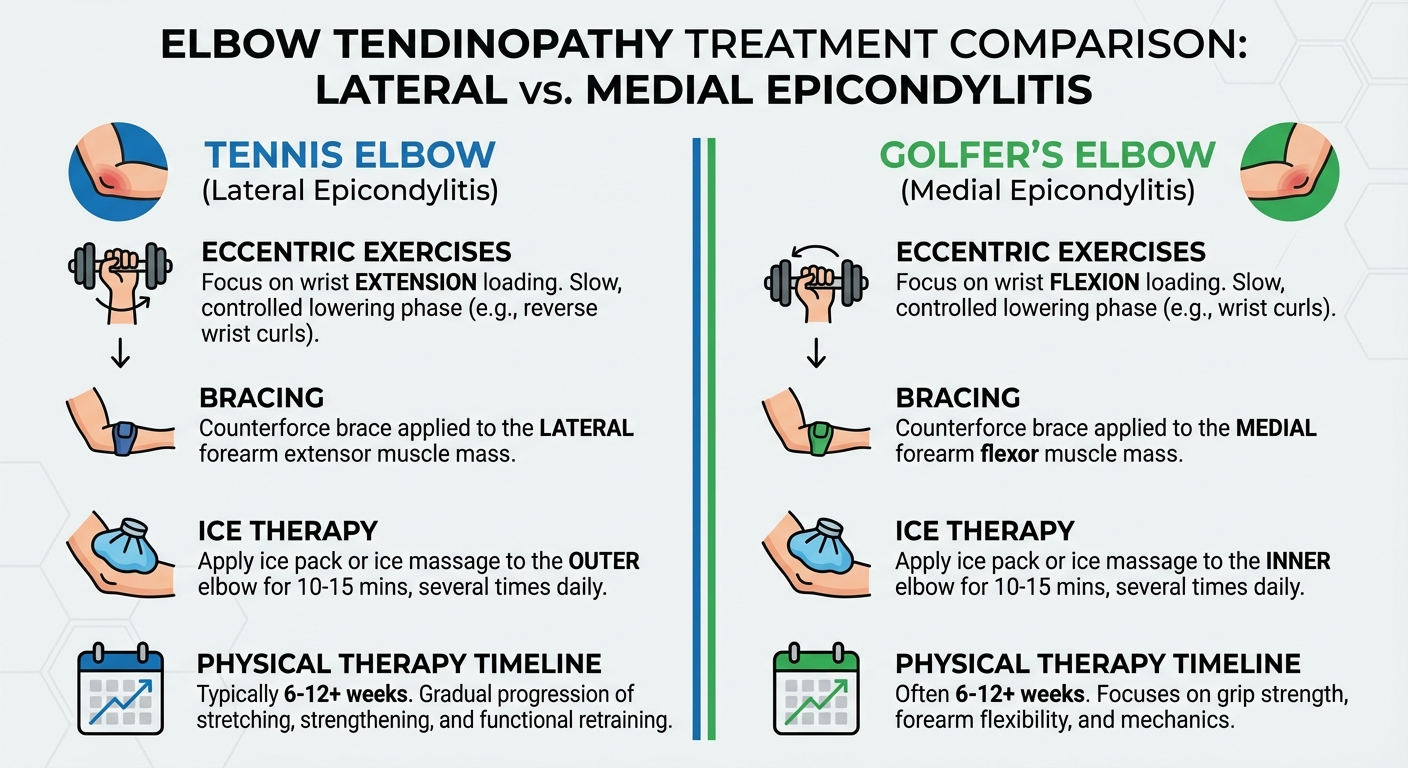
The good news is that both tennis elbow and golfer's elbow respond well to conservative (non-surgical) treatment in the vast majority of cases. Treatment principles overlap significantly, though some specifics differ.
Phase 1: Acute Pain Management (Weeks 1-4)
- Relative rest: Avoid the aggravating activity, but do not immobilize the arm completely. Complete rest leads to muscle atrophy and tendon weakening
- Ice: Apply for 15-20 minutes several times daily to manage pain
- NSAIDs: Short-term use (1-2 weeks) of ibuprofen or naproxen can help with acute pain. Not recommended long-term as they may impair tendon healing
- Counterforce bracing: A tennis elbow strap worn just below the elbow can offload the tendon during daily activities. Finding the best tennis elbow brace for your situation can significantly reduce pain during this phase
Recommended Tennis Elbow Braces:
Browse Top-Rated Tennis Elbow Braces on Amazon
Browse Top-Rated Golfer's Elbow Braces on Amazon
Phase 2: Rehabilitation (Weeks 4-12)
This is the most critical phase. Progressive loading through eccentric and isometric exercises is the gold standard for tendon rehabilitation.
For Tennis Elbow:
- Tyler Twist with FlexBar: The single most evidence-backed exercise for lateral epicondylitis. Studies show a 72% improvement in pain scores over 8 weeks
- Eccentric wrist extensions: Slowly lowering a light dumbbell with the forearm pronated (palm down)
- Isometric wrist extension holds: Holding a light weight in wrist extension for 30-45 seconds
Browse FlexBar Resistance Bars on Amazon
For Golfer's Elbow:
- Reverse Tyler Twist: The FlexBar exercise performed in reverse, loading the flexor tendons eccentrically
- Eccentric wrist curls: Slowly lowering a light dumbbell with the forearm supinated (palm up)
- Forearm pronation/supination: Controlled rotation exercises with a light weight or hammer
Phase 3: Return to Activity (Months 3-6+)
- Gradual reintroduction: Slowly return to the aggravating activity, increasing load by no more than 10-15% per week
- Technique correction: Address any biomechanical faults that contributed to the injury. For tennis players, this may mean adjusting grip size, string tension, or backhand technique
- Strength and conditioning: Build global upper extremity strength to distribute forces more evenly
Advanced Treatments
When conservative care fails after 6-12 months, more advanced interventions may be considered:
- Platelet-rich plasma (PRP) injections: Growing evidence supports PRP for chronic tendinopathy, though results are mixed
- Shockwave therapy (ESWT): Extracorporeal shockwave therapy stimulates a healing response in degenerated tendons. Multiple studies show moderate benefit
- Corticosteroid injections: Provide short-term relief (2-6 weeks) but are associated with worse long-term outcomes and higher recurrence rates. Most experts now advise against them except for acute pain management
- Surgery: Reserved for the 5-10% of cases that fail all conservative measures after 6-12 months. Surgical debridement of the degenerated tendon tissue has an 80-90% success rate
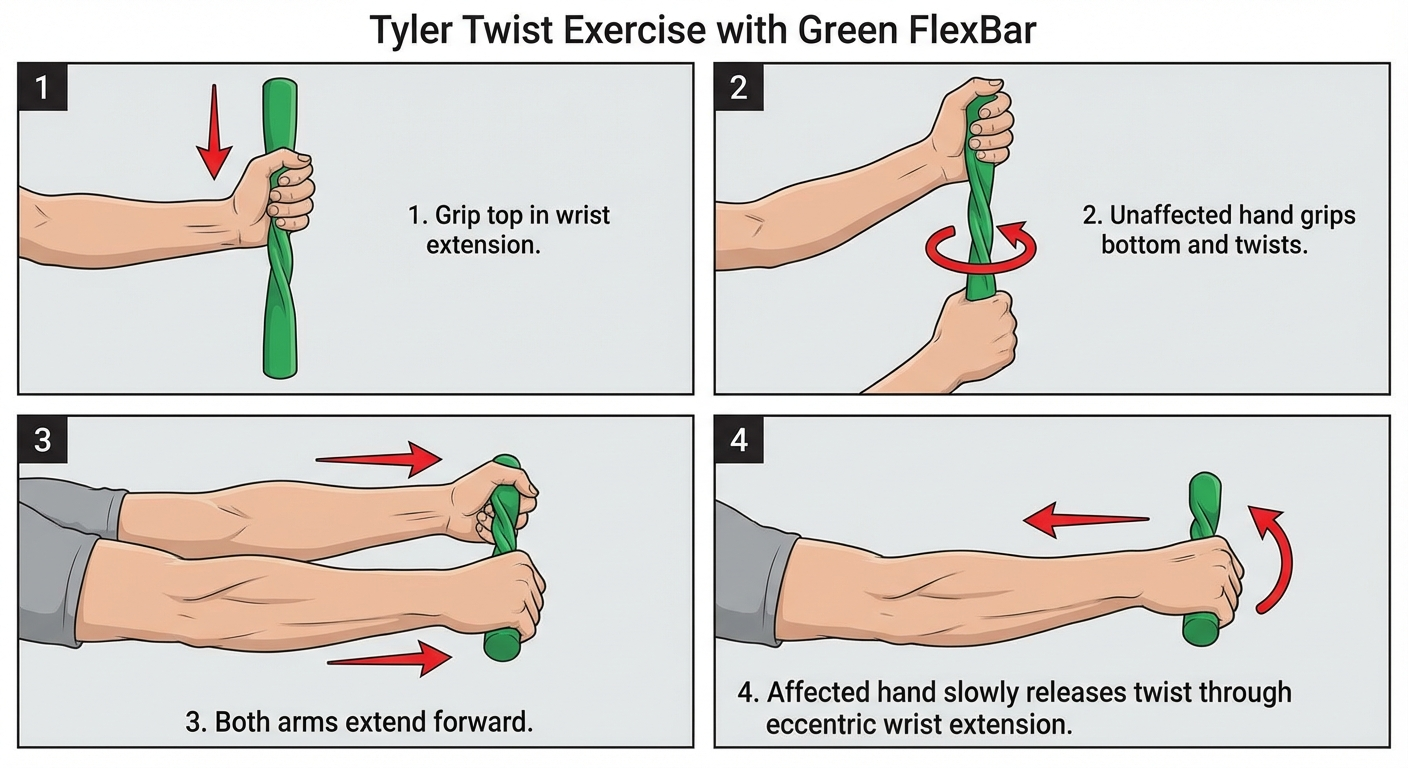 The Tyler Twist is the gold standard eccentric exercise for lateral epicondylitis — studies show 80%+ success rate at 6 weeks.
The Tyler Twist is the gold standard eccentric exercise for lateral epicondylitis — studies show 80%+ success rate at 6 weeks.
 A counterforce brace reduces tendon load during activities — it's a short-term tool, not a cure. Combine with eccentric exercises for lasting results.
A counterforce brace reduces tendon load during activities — it's a short-term tool, not a cure. Combine with eccentric exercises for lasting results.
Which Heals Faster?
This is one of the most common questions patients ask, and the honest answer is that both conditions have similar recovery timelines. Most cases of tennis elbow and golfer's elbow resolve within 6 to 24 months with appropriate conservative management.
However, there are some nuances worth considering:
- Golfer's elbow may have a slight edge in recovery speed for some patients, possibly because the medial epicondyle has a slightly better blood supply than the lateral epicondyle. However, this difference is modest and not consistently demonstrated in research
- Tennis elbow has higher recurrence rates, estimated at 8-15% within the first year after resolution. This may be because the aggravating activities (computer work, daily gripping tasks) are harder to avoid compared to sport-specific triggers for golfer's elbow
- Compliance with rehabilitation is the strongest predictor of recovery speed for both conditions. Patients who perform their eccentric loading program consistently tend to recover months faster than those who rely solely on passive treatments like bracing or injections
The bottom line: do not expect one condition to heal dramatically faster than the other. Focus on consistent rehabilitation and gradual return to activity regardless of which diagnosis you have.
Can You Have Both at the Same Time?
Yes, you can have both tennis elbow and golfer's elbow simultaneously, though it is relatively uncommon. This scenario is most likely in people who perform heavy, repetitive gripping tasks that load both the extensor and flexor muscle groups. Manual laborers, rock climbers, and CrossFit athletes are among those most at risk for concurrent lateral and medial epicondylitis.
When both conditions are present, treatment follows the same principles, but rehabilitation must address both tendon groups. This typically means performing both eccentric wrist extension and eccentric wrist flexion exercises, and being particularly careful about load management during recovery.
If you are experiencing pain on both sides of your elbow, it is especially important to see a healthcare provider. Pain on both the medial and lateral aspects of the elbow can sometimes indicate a more systemic issue, such as inflammatory arthritis or a referred pain pattern from the cervical spine, rather than simple overuse tendinopathy.
 Prevention is always better than treatment — strengthen wrist extensors and flexors before injury occurs.
Prevention is always better than treatment — strengthen wrist extensors and flexors before injury occurs.
Prevention Strategies
Whether you have recovered from epicondylitis or want to avoid it entirely, these strategies reduce your risk:
Equipment and Ergonomics
- Use proper grip size: A grip that is too small or too large increases tendon load. For racquet sports, your ideal grip allows a finger's width between your fingertips and palm
- Ergonomic workspace: Keep your wrist in a neutral position while typing. Use an ergonomic mouse and consider a vertical mouse design
- Vibration dampening: If you use power tools, invest in anti-vibration gloves and tools with dampening features
Browse Ergonomic Mouse Options on Amazon
Training Principles
- Progress gradually: Follow the 10% rule — increase training volume or intensity by no more than 10% per week
- Warm up properly: Dynamic stretching of the forearm extensors and flexors before activity
- Strengthen the full chain: Do not neglect shoulder and scapular stability. Weakness in the shoulder forces the forearm muscles to compensate
- Cross-train: Vary your activities to avoid repetitive strain on the same tendon groups
Ongoing Maintenance
- Regular eccentric exercises: Even after recovery, performing maintenance sets of eccentric wrist exercises 2-3 times per week can help prevent recurrence
- Self-massage and foam rolling: Forearm soft tissue work with a lacrosse ball can improve blood flow and reduce muscle tightness
- Listen to your body: Mild elbow soreness after activity that resolves within 24 hours is acceptable. Pain that persists or worsens is a warning sign to reduce load
When to See a Doctor
While many cases of epicondylitis can be managed with self-directed rehabilitation, you should seek professional evaluation if:
- Pain persists for more than 2-4 weeks despite rest and home treatment
- You are unable to perform daily activities such as lifting a coffee cup, turning a doorknob, or typing
- You experience numbness, tingling, or weakness in your hand or fingers
- The elbow appears swollen, red, or warm to the touch (this may indicate a different condition)
- You have a history of elbow injury, surgery, or inflammatory conditions
- Your symptoms are getting progressively worse rather than improving
- You have pain on both the inside and outside of your elbow
A sports medicine physician, orthopedic surgeon, or physiotherapist with experience in upper extremity conditions can provide an accurate diagnosis and personalized treatment plan.
Frequently Asked Questions
Is tennis elbow worse than golfer's elbow?
Neither condition is inherently "worse" than the other. Tennis elbow is roughly 5-10 times more common, which may create the perception that it is more severe. Both can range from mild discomfort to significant disability depending on the degree of tendon degeneration. The severity depends on factors like how long the condition has been present, your overall health, and whether you continue the aggravating activity.
Can I still exercise with tennis elbow or golfer's elbow?
Yes, but you need to modify your training. Avoid exercises that directly aggravate your symptoms. Lower body training is generally fine. For upper body work, reduce grip-intensive exercises and focus on movements that do not provoke pain. Many people can continue training throughout their recovery by making smart substitutions and reducing load on the affected tendons.
How do I know if I have tennis elbow or golfer's elbow without seeing a doctor?
The simplest way is to locate your pain. Press on the bony bump on the outside of your elbow — if this is tender, it suggests tennis elbow. Press on the bony bump on the inside — if this is tender, it suggests golfer's elbow. You can also perform the Cozen's and reverse Cozen's tests described earlier in this article. However, a professional diagnosis is always recommended to rule out other conditions.
Do cortisone shots work for tennis elbow or golfer's elbow?
Cortisone (corticosteroid) injections provide short-term pain relief lasting 2-6 weeks, but research consistently shows worse long-term outcomes compared to physical therapy alone. A landmark 2013 study in The Lancet found that patients who received cortisone injections had significantly higher recurrence rates at one year compared to those who did physiotherapy or watchful waiting. Most sports medicine experts now recommend against routine cortisone use for epicondylitis.
What is the fastest way to cure tennis elbow?
There is no instant cure for tennis elbow. The fastest path to recovery involves early intervention with a progressive eccentric exercise program (such as the Tyler Twist with a FlexBar), activity modification to reduce tendon load, and patience. Most patients see meaningful improvement within 6-12 weeks of consistent rehabilitation. Trying to rush recovery by ignoring pain or relying solely on passive treatments like bracing typically leads to a longer overall recovery.
Can tennis elbow or golfer's elbow become permanent?
In rare cases, chronic epicondylitis can persist for years if left untreated or if the aggravating activity is not modified. However, with appropriate treatment — including eccentric loading exercises and, if necessary, advanced interventions like PRP or surgery — the vast majority of patients achieve full or near-full recovery. Fewer than 5% of patients require surgical intervention.
---## Sources
-
Bisset, L., Beller, E., Jull, G., Brooks, P., Darnell, R., & Vicenzino, B. (2006). Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ, 333(7575), 939. https://doi.org/10.1136/bmj.38961.584653.AE
-
Coombes, B.K., Bisset, L., & Vicenzino, B. (2013). Management of lateral elbow tendinopathy: one size does not fit all. The Lancet, 382(9897), 1084-1086. https://doi.org/10.1016/S0140-6736(13)61693-2
-
Tyler, T.F., Thomas, G.C., Nicholas, S.J., & McHugh, M.P. (2010). Addition of isolated wrist extensor eccentric exercise to standard treatment for chronic lateral epicondylosis: a prospective randomized trial. Journal of Shoulder and Elbow Surgery, 19(6), 917-922. https://doi.org/10.1016/j.jse.2010.04.041
-
Shiri, R., Viikari-Juntura, E., Varonen, H., & Heliövaara, M. (2006). Prevalence and determinants of lateral and medial epicondylitis: a population study. American Journal of Epidemiology, 164(11), 1065-1074. https://doi.org/10.1093/aje/kwj325
Walking Pad vs Treadmill
30-second comparison