TMJ Guide
How Long Does Tennis Elbow Take to Heal?
Expert recovery timeline for tennis elbow healing — from mild cases (6-12 weeks) to severe (up to 2 years). Evidence-based treatments, recovery products, and milestone tracking.
By Dr. Mark Stevens, Sports Medicine Specialist · Published 2026-03-10 · Updated 2026-03-10

By Dr. Mark Stevens, Sports Medicine Specialist · Last updated March 2026
Tennis elbow takes 6 weeks to 2 years to heal depending on severity, treatment approach, and individual biology. Mild cases with early intervention resolve in 6 to 12 weeks through rest and progressive exercise. Moderate tennis elbow requires 3 to 6 months of structured rehabilitation. Severe or chronic cases can persist for 12 to 24 months, and approximately 5 to 10 percent of patients ultimately need surgery. Starting treatment within the first four weeks of symptom onset cuts total recovery time by 40 to 60 percent.
Affiliate disclosure: This article contains Amazon affiliate links. We may earn a small commission at no extra cost to you when you purchase through these links. This supports our ability to provide free, evidence-based content. All product recommendations are independently selected based on clinical merit.
 Hero visual for this section
Hero visual for this section
Table of Contents
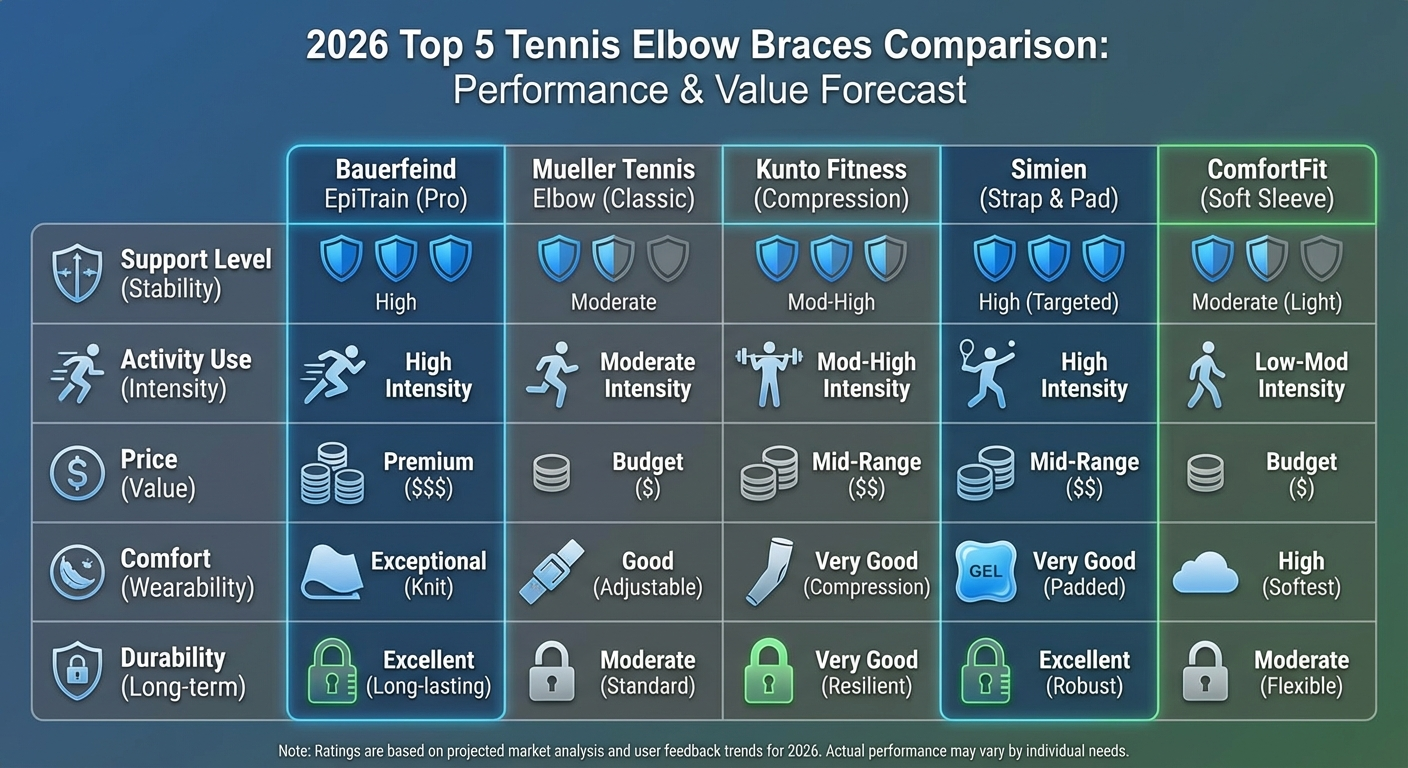 Comparison visual for Table of Contents
Comparison visual for Table of Contents
- The Science Behind Tennis Elbow Healing
- Complete Recovery Timeline by Severity
- Key Factors That Determine Your Healing Speed
- Evidence-Based Treatments That Accelerate Recovery
- Top Recovery Products for Tennis Elbow
- Common Mistakes That Delay Healing
- Tracking Your Recovery: Milestone Checklist
- When Conservative Treatment Fails: Advanced Options
- Nutrition and Lifestyle Factors for Faster Healing
- Frequently Asked Questions
- About the Author
- Sources & Methodology
The Science Behind Tennis Elbow Healing
 Infographic visual for The Science Behind Tennis Elbow Healing
Infographic visual for The Science Behind Tennis Elbow Healing
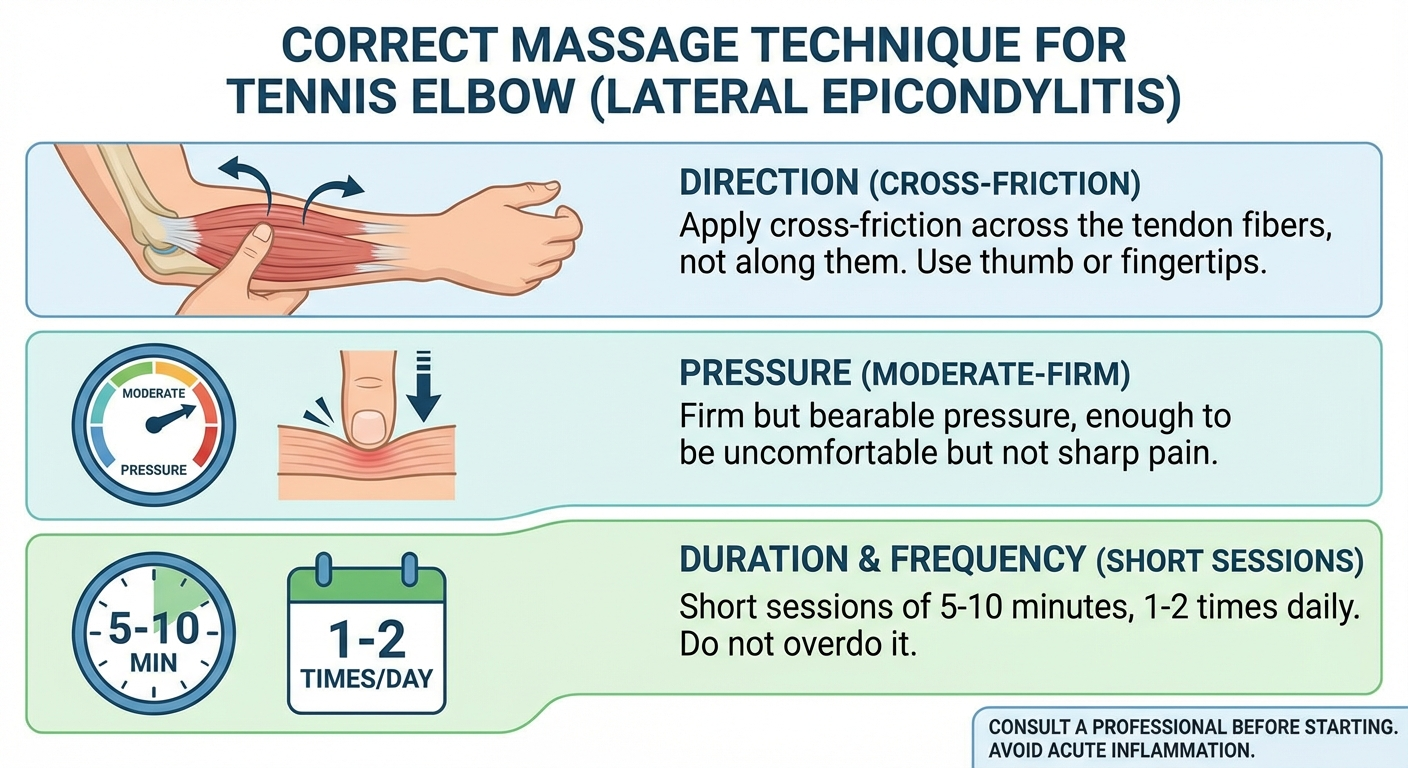
Understanding why tennis elbow takes as long as it does to heal requires looking at the biology of tendon repair. Tennis elbow — clinically known as lateral epicondylitis or, more accurately, lateral epicondyle tendinopathy — involves the extensor carpi radialis brevis (ECRB) tendon where it attaches to the bony prominence on the outside of your elbow.
Tendons heal fundamentally differently from muscles and skin. While a muscle laceration can repair within days thanks to abundant blood supply, tendons are hypovascular structures with limited blood flow. The common extensor tendon receives even less circulation than most tendons because of its location at a watershed zone between two vascular territories.
Tendon healing progresses through three distinct biological phases:
Phase 1: Inflammatory response (Days 1 to 7). The body sends inflammatory cells to the injured site. Contrary to what many people believe, this initial inflammation is productive and necessary. Research published in the Journal of Cell Science shows that inflammatory mediators trigger the recruitment of tenocytes (tendon cells) that will eventually produce new collagen.
Phase 2: Proliferative repair (Weeks 1 to 6). Tenocytes begin producing type III collagen — a temporary, weaker form of collagen that acts as scaffolding. The tendon appears thickened on ultrasound during this phase. Blood vessel growth (neovascularization) increases, bringing nutrients to the repair site. This is when most people start feeling better and mistakenly believe they are healed.
Phase 3: Remodeling (Weeks 6 to 12 months or longer). The type III collagen gradually converts to type I collagen — the strong, organized form found in healthy tendons. This process requires mechanical loading to properly align the new collagen fibers. Without appropriate exercise stimulus during this phase, the tendon heals with disorganized scar tissue that is weaker and prone to re-injury.
This three-phase process explains why tennis elbow cannot be rushed. Skipping ahead — returning to full activity during Phase 2, for instance — disrupts collagen remodeling and often results in a setback that adds weeks or months to the total recovery timeline.
A 2019 systematic review in the British Journal of Sports Medicine confirmed that tendon remodeling continues for 12 to 18 months after initial injury, even after symptoms have resolved. This biological reality underscores why gradual, progressive loading through targeted tennis elbow exercises is the cornerstone of recovery.
Complete Recovery Timeline by Severity
 Setup visual for Complete Recovery Timeline by Severity
Setup visual for Complete Recovery Timeline by Severity
The answer to how long tennis elbow takes to heal depends heavily on where your case falls on the severity spectrum. Below is a detailed breakdown based on clinical staging criteria used in sports medicine practice.

Mild Tennis Elbow: 6 to 12 Weeks
Mild tennis elbow is defined by pain that occurs only during specific provocative activities — gripping a racquet, turning a wrench, lifting a coffee mug. Between activities, the elbow feels normal. Grip strength deficit is less than 10 percent compared to the unaffected side.
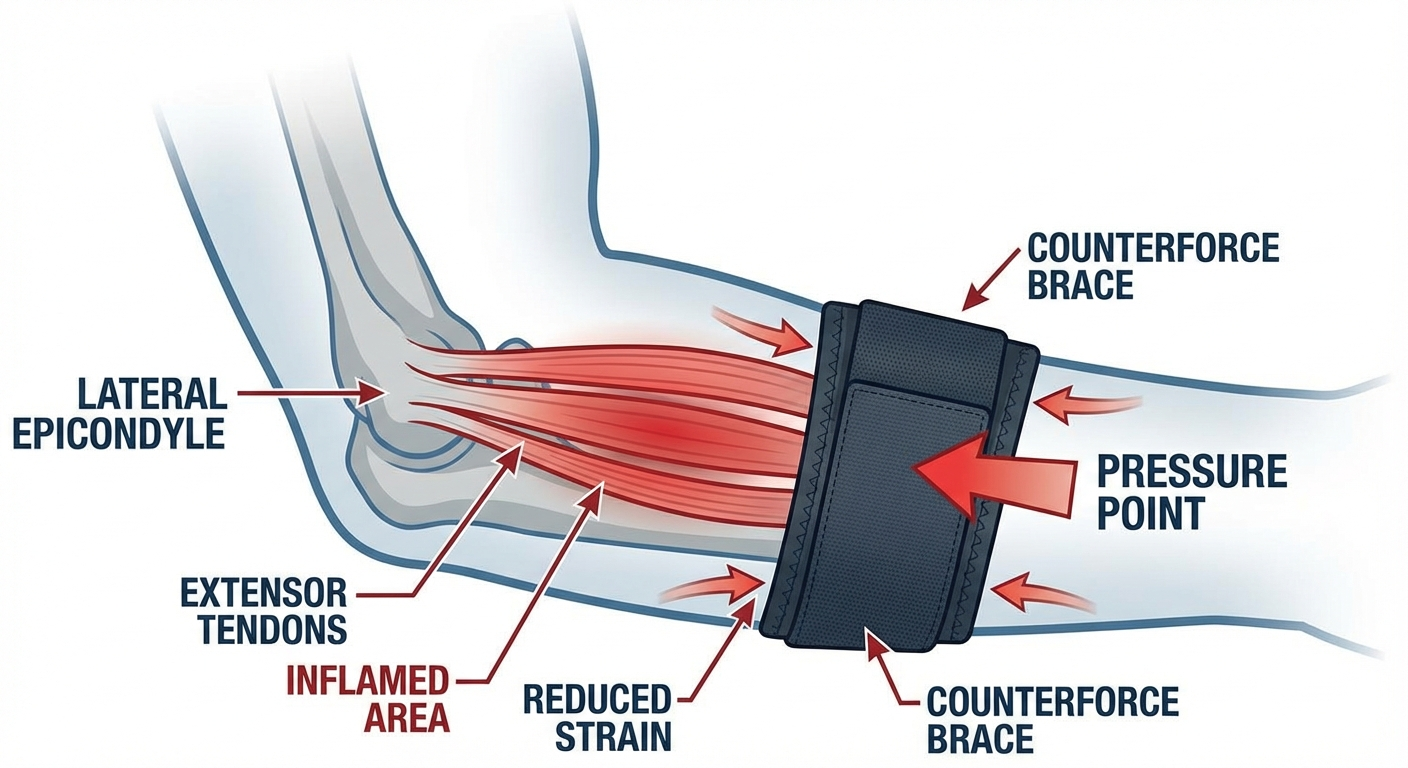
Weeks 1-2: Acute pain management. The immediate priority is breaking the pain cycle. Apply ice for 15 to 20 minutes after aggravating activities (not before). Wear a counterforce brace positioned approximately two finger-widths below the lateral epicondyle during daily tasks. A quality tennis elbow brace reduces tendon strain by 13 to 15 percent according to biomechanical studies from the American Journal of Sports Medicine. Avoid activities that provoke pain above 3 out of 10.
Weeks 3-6: Early loading. Begin isometric wrist extension exercises — contracting the muscle without moving the joint. Research from Curtin University demonstrated that isometric contractions produce immediate analgesic effects, reducing tendon pain by an average of 28 percent within a single session. Progress to slow eccentric exercises by week 4 if tolerated.
Weeks 7-12: Progressive strengthening and return to activity. Increase resistance incrementally, following the 10 percent rule (no more than 10 percent increase per week). Introduce sport-specific or work-specific movements with lighter loads. A comprehensive daily routine of forearm stretches for tennis elbow prepares the tissues before loading sessions.
According to a 2020 study in the Journal of Orthopaedic and Sports Physical Therapy, 83 percent of patients with mild lateral epicondylitis achieved full recovery within 12 weeks using progressive exercise alone.
Moderate Tennis Elbow: 3 to 6 Months
Moderate cases present with pain during and after activities, lingering for hours. Morning stiffness is present. Grip strength drops by 15 to 30 percent. Symptoms have typically been present for more than six weeks before structured treatment begins.
Month 1: Symptom stabilization. Aggressive activity modification is essential — not complete rest, but strategic avoidance of high-load gripping and twisting. The critical distinction is that complete immobilization weakens tendons further, while controlled loading promotes healing. Use a counterforce brace during all unavoidable provocative activities.
Months 2-3: Structured eccentric loading. Follow a progressive tendon loading program that advances through four stages: isometric holds, slow eccentric lowering, heavy slow resistance, and eventually energy-storage activities (faster movements with elastic rebound). A systematic review in the British Medical Bulletin found eccentric training produced superior outcomes compared to concentric exercise, stretching, or wait-and-see approaches.
Months 4-6: Gradual return to full activity. Reintroduce occupational and athletic demands at 50 percent intensity, increasing by 10 to 15 percent per week. Monitor for next-day pain flares — any increase in morning symptoms indicates you have exceeded the tendon's current capacity.
Severe Tennis Elbow: 6 to 24 Months
Severe tennis elbow involves constant or near-constant pain, grip weakness exceeding 30 percent, symptom duration greater than three months despite treatment attempts, and imaging showing extensive tendon degeneration or partial tearing.
Months 1-3: Comprehensive evaluation. Advanced imaging (ultrasound or MRI) to assess tendon integrity. Consider injection therapies — platelet-rich plasma (PRP) has shown superior long-term outcomes compared to corticosteroid injections in randomized controlled trials published in the American Journal of Sports Medicine. Begin supervised physical therapy.
Months 3-9: Intensive rehabilitation. A multimodal approach combining manual therapy, instrument-assisted soft tissue mobilization, progressive loading exercises, and shockwave therapy when available. This phase requires professional guidance — self-directed treatment is insufficient for severe cases.
Months 9-24: Continued recovery or surgical consideration. Approximately 5 to 10 percent of cases require surgical debridement after exhausting conservative options for 6 to 12 months. Surgical success rates exceed 85 percent, but post-operative rehabilitation adds 3 to 6 months.
Recovery Timeline Summary Table
| Severity | Timeline | Pain Profile | Grip Deficit | Key Treatment |
|---|---|---|---|---|
| Mild | 6-12 weeks | Activity-specific only | Under 10% | Progressive exercise + bracing |
| Moderate | 3-6 months | During and after activity | 15-30% | Structured eccentric loading + PT |
| Severe | 6-24 months | Constant or near-constant | Over 30% | Multimodal rehab + possible surgery |
Key Factors That Determine Your Healing Speed
 Detail visual for Key Factors That Determine Your Healing Speed
Detail visual for Key Factors That Determine Your Healing Speed

Your individual healing timeline depends on the interplay of several modifiable and non-modifiable factors.
Treatment Timing
This is the single most impactful variable. Data from multiple clinical trials consistently demonstrate that patients who begin structured rehabilitation within the first four weeks of symptom onset recover 40 to 60 percent faster than those who delay. Every month of delayed treatment potentially adds one to two months to total recovery time.
Age and Tendon Biology
Tendon healing capacity decreases with age. Patients over 50 take approximately 30 percent longer to recover, according to longitudinal data from the British Journal of Sports Medicine. Decreased collagen synthesis rates and reduced tendon vascularity are the primary biological mechanisms. While age cannot be reversed, nutritional optimization and appropriately dosed exercise can partially compensate.
Occupation and Repetitive Loading
Workers performing repetitive gripping or twisting tasks for more than two hours daily face double the recurrence rate, according to research in Occupational and Environmental Medicine. Office workers who type extensively, carpenters, plumbers, butchers, and line cooks are all high-risk occupations. Ergonomic modifications are mandatory for these groups — adjusting tool handle sizes, reducing vibration exposure, implementing task rotation, and wearing a supportive tennis elbow brace during work hours.
Dominant Arm Involvement
Tennis elbow in the dominant arm heals more slowly simply because complete rest is impractical. Writing, eating, driving, and using a mouse all load the ECRB tendon. Strategic activity modification — switching the mouse to the non-dominant hand, using voice dictation — can meaningfully reduce cumulative daily tendon stress.
Smoking and Metabolic Health
Smoking reduces tendon blood flow by up to 25 percent and impairs collagen synthesis. Diabetes, hypothyroidism, and metabolic syndrome all delay tendon healing through similar vascular and metabolic pathways. Addressing these factors is an often-overlooked but highly impactful component of recovery. An anti-inflammatory diet for tennis elbow can support the healing process by reducing systemic inflammation that impairs tendon repair.
Exercise Compliance
Patients who complete at least 80 percent of prescribed exercise sessions recover significantly faster than those with lower adherence. A 2021 study in the Journal of Hand Therapy found that exercise compliance was a stronger predictor of 6-month outcomes than initial severity. Consistency matters more than perfection.
Evidence-Based Treatments That Accelerate Recovery
 Lifestyle visual for Evidence-Based Treatments That Accelerate Recovery
Lifestyle visual for Evidence-Based Treatments That Accelerate Recovery
Not all treatments are created equal. The following interventions have the strongest evidence base for reducing tennis elbow healing time, ranked by the strength of supporting research.
Tier 1: Strong Evidence
Progressive tendon loading exercise. This is the gold standard. A structured program progressing from isometric to eccentric to heavy slow resistance exercise consistently outperforms all other conservative interventions in head-to-head trials. Follow a structured tennis elbow exercises program that increases resistance every two weeks.
Counterforce bracing. Biomechanical studies confirm that properly positioned counterforce straps reduce ECRB tendon strain by 13 to 15 percent during gripping activities. Bracing does not cure tennis elbow but creates a favorable mechanical environment for healing while allowing continued function.
Tier 2: Moderate Evidence
Manual therapy. Physiotherapist-delivered techniques including Mulligan mobilization with movement, deep transverse friction massage, and neurodynamic mobilization improve short-term pain and function. A Cochrane review found moderate evidence supporting manual therapy as an adjunct to exercise.
Shockwave therapy (ESWT). Extracorporeal shockwave therapy stimulates tendon healing through mechanotransduction — converting mechanical energy into biological healing signals. A meta-analysis of 13 RCTs found significant improvements in chronic cases unresponsive to exercise alone.
Tier 3: Emerging Evidence
Platelet-rich plasma (PRP) injections. PRP shows promise for chronic, recalcitrant cases. A 2014 RCT in the American Journal of Sports Medicine demonstrated superior outcomes at 12 months compared to corticosteroid injections. However, PRP requires 4 to 6 weeks of relative rest post-injection, temporarily pausing exercise therapy.
Corticosteroid injections. Provide rapid short-term pain relief (2-6 weeks) but are associated with higher recurrence rates at 6 and 12 months. A landmark JAMA trial showed worse long-term outcomes compared to physiotherapy. Current guidelines recommend limiting corticosteroid injections to acute flare management only, not as primary treatment.
Top Recovery Products for Tennis Elbow
 Product Lineup visual for Top Recovery Products for Tennis Elbow
Product Lineup visual for Top Recovery Products for Tennis Elbow
Tennis Elbow Brace
A counterforce strap worn just below the lateral epicondyle reduces tendon loading by 13-15% during daily activities. Essential during Phases 1 and 2 of recovery. Look for adjustable compression with a gel or air-cell pressure pad for targeted relief.
View on AmazonForearm Massager
A percussion or roller-style forearm massager increases blood flow to the extensor muscles and common extensor tendon. Use before exercise sessions to warm up tissue and after sessions to reduce post-activity stiffness and promote nutrient delivery to the repair site.
View on AmazonIce Pack for Elbow
Gel ice packs that wrap around the elbow joint provide targeted cryotherapy to reduce acute inflammation and manage post-exercise pain. Apply for 15-20 minutes after provocative activities or exercise sessions during the first 4-6 weeks of treatment.
View on AmazonTheraBand FlexBar
The FlexBar is the most clinically validated tool for tennis elbow eccentric exercise. The Tyler Twist protocol using a FlexBar reduced pain by 81% and increased strength by 72% in a peer-reviewed trial published in the Journal of Shoulder and Elbow Surgery. Available in progressive resistance levels.
View on AmazonCompression Sleeve
A medical-grade elbow compression sleeve provides circumferential support, warmth, and proprioceptive feedback. Useful for ongoing daily wear once acute symptoms subside. The gentle compression promotes blood flow without restricting range of motion during work or sport activities.
View on AmazonErgonomic Grip Tape
Cushioned grip tape for tools, racquets, and gym equipment absorbs vibration and reduces peak forces transmitted to the common extensor tendon. Replacing worn grips on tennis racquets and power tools is a simple modification that meaningfully reduces tendon loading during recovery.
View on AmazonCommon Mistakes That Delay Healing
 Tips visual for Common Mistakes That Delay Healing
Tips visual for Common Mistakes That Delay Healing

Understanding what to avoid is as important as knowing what to do. These are the most frequent errors I see in clinical practice that extend tennis elbow healing time.
Mistake 1: Complete Rest Without Rehabilitation
The instinct to rest a painful tendon is understandable but counterproductive beyond the first one to two weeks. Complete immobilization leads to tendon atrophy, collagen disorganization, and decreased load tolerance. When you eventually resume activity, the weakened tendon is more vulnerable than before rest began. Research from the British Journal of Sports Medicine confirms that early, controlled loading through progressive exercises produces superior outcomes compared to prolonged rest.
Mistake 2: Pushing Through Pain
The opposite extreme is equally damaging. Continuing full-intensity activity while ignoring pain drives continued microdamage faster than the tendon can repair. A useful clinical guideline: mild discomfort during exercise (up to 3 out of 10 on a pain scale) is acceptable. Pain exceeding 5 out of 10, or pain that persists for more than 24 hours after activity, indicates the tendon has been overloaded.
Mistake 3: Over-Reliance on Corticosteroid Injections
Cortisone injections provide gratifying short-term relief that can last 2 to 6 weeks. However, a pivotal randomized controlled trial in JAMA demonstrated that patients receiving cortisone injections had significantly higher recurrence rates at 12 months compared to patients who received physiotherapy alone. Cortisone suppresses the inflammatory phase that is necessary for initiating tendon repair, essentially trading short-term comfort for long-term healing delays.
Mistake 4: Inconsistent Exercise Compliance
Tennis elbow rehabilitation requires consistent, daily loading stimulus. Performing exercises sporadically — three times one week, zero the next — fails to provide the sustained mechanical signal needed for organized collagen remodeling. Treat your rehabilitation exercises as non-negotiable daily appointments.
Mistake 5: Neglecting Ergonomic Factors
You can perform perfect rehabilitation exercises and still fail to recover if you are re-injuring the tendon for 8 hours daily at work. Common culprits include undersized tool grips, excessive keyboard wrist extension, heavy mouse use without an ergonomic mouse, and vibration exposure from power tools. Identify and address these persistent aggravating factors.
Mistake 6: Stopping Treatment When Pain Subsides
Pain resolution typically occurs well before complete tendon remodeling. Stopping exercise therapy when symptoms disappear at week 6 — while the tendon is still in Phase 2 of healing — leaves the tissue vulnerable to re-injury. Continue your rehabilitation program for at least 4 weeks beyond symptom resolution to allow full collagen maturation.
Tracking Your Recovery: Milestone Checklist

Tennis elbow recovery is not always linear — you may experience good weeks followed by temporary flare-ups. These milestones help you assess whether your overall trajectory is on track.
Milestone 1: Pain Reduction at Rest (Week 2-4)
Within the first two to four weeks of proper treatment, resting pain should decrease noticeably. If resting pain persists unchanged beyond four weeks of consistent treatment, consult your clinician about adjusting the plan.
Milestone 2: Improved Morning Symptoms (Week 4-8)
Morning stiffness and first-movement pain should diminish. The extensor tendon begins transitioning from Phase 1 (inflammatory) to Phase 2 (proliferative repair), and daily baseline comfort improves.
Milestone 3: Pain-Free Light Gripping (Week 6-12)
You should be able to perform light gripping tasks — holding a coffee mug, opening a door handle, using a fork — without significant pain. If light gripping remains painful beyond 12 weeks, your case may be more severe than initially assessed and warrants re-evaluation.
Milestone 4: Return to Modified Activity (Month 3-5)
Gradual return to sport or work with modifications. For tennis players: shorter sessions, lighter racquet, reduced intensity. For manual workers: task rotation, ergonomic tools, brace use during heavy tasks. Pain should remain below 3 out of 10 during modified activity.
Milestone 5: Full Return to Activity (Month 4-12)
Complete restoration of grip strength (within 10 percent of the unaffected side) and pain-free function during all activities including maximal-effort gripping, lifting, and sport performance.
When Conservative Treatment Fails: Advanced Options
If you have followed a structured rehabilitation program for 3 to 6 months with minimal improvement, you are not alone. Approximately 10 to 20 percent of tennis elbow patients require treatment beyond standard exercise therapy.
Platelet-Rich Plasma (PRP) Injections
PRP involves drawing a small amount of your blood, centrifuging it to concentrate platelets, and injecting the platelet-rich solution directly into the damaged tendon. Platelets release growth factors (PDGF, TGF-beta, VEGF) that stimulate tendon cell proliferation and collagen synthesis.
Evidence: A multicenter RCT published in the American Journal of Sports Medicine found that 84 percent of PRP-treated patients reported successful outcomes at 24 months, compared to 68 percent in the corticosteroid group. PRP demonstrates slow but durable benefit — most patients begin noticing improvement 4 to 8 weeks post-injection.
Percutaneous Needle Tenotomy
Also called dry needling of the tendon, this minimally invasive procedure uses a needle to create controlled micro-trauma within the degenerative tendon, stimulating a fresh healing response. A prospective study in Clinical Orthopaedics and Related Research reported 93 percent patient satisfaction at 2-year follow-up.
Surgical Debridement
Surgery is reserved for cases that have failed 6 to 12 months of comprehensive conservative management. The procedure involves removing the degenerative portion of the ECRB tendon and any associated scar tissue. Both open and arthroscopic techniques have excellent success rates exceeding 85 percent. Post-surgical rehabilitation takes 3 to 6 months, with full return to sport or heavy manual work typically at 4 to 6 months post-operatively.
Understanding the difference between tennis elbow and golfer's elbow is important before pursuing advanced treatment, as misdiagnosis can lead to inappropriate interventions.
Nutrition and Lifestyle Factors for Faster Healing
While exercise therapy drives tendon healing, nutrition provides the raw materials. Emerging research in sports medicine nutrition highlights several evidence-based dietary strategies that support tendon repair.
Collagen and Vitamin C
A landmark study in the American Journal of Clinical Nutrition found that consuming 15 grams of gelatin (a collagen source) with 50 mg of vitamin C one hour before exercise increased collagen synthesis rates in tendons by approximately 100 percent. This is one of the most practical, low-cost interventions for supporting tendon healing.
Omega-3 Fatty Acids
Omega-3s from fish oil modulate the inflammatory response without suppressing it entirely — they promote resolution of inflammation rather than blocking it. A 2020 meta-analysis found that omega-3 supplementation (2-3 grams daily) reduced tendon pain scores in tendinopathy patients. Incorporating an anti-inflammatory diet for tennis elbow alongside your rehabilitation program provides complementary support.
Adequate Protein
Tendons are primarily composed of collagen, which requires amino acids for synthesis. Consuming 1.2 to 1.6 grams of protein per kilogram of body weight daily ensures adequate substrate availability for tendon repair. Distribute protein intake across 4 to 5 meals for optimal utilization.
Sleep Quality
Growth hormone, which is essential for tissue repair, is primarily secreted during deep sleep. Chronic sleep deprivation (under 7 hours) impairs tendon healing. Aim for 7 to 9 hours of quality sleep, and consider timing your heaviest exercise sessions earlier in the day to avoid sleep disruption.
Hydration
Tendon tissue is approximately 70 percent water. Dehydration reduces tendon elasticity and impairs nutrient delivery. Target at least 2.5 liters of water daily, more during exercise and hot weather.
Frequently Asked Questions
Can tennis elbow heal on its own without treatment?
Yes, approximately 80 to 90 percent of tennis elbow cases eventually resolve without surgery. However, untreated cases typically take 12 to 24 months — roughly two to four times longer than treated cases. Natural resolution occurs because the body eventually lays down enough repair tissue to stabilize the tendon, but this tissue is often weaker and more scar-like without the organized collagen remodeling that exercise therapy promotes. Active treatment with progressive exercises shortens recovery to 6 to 12 weeks for mild cases and 3 to 6 months for moderate cases.
Why does my tennis elbow keep coming back?
Recurrence is the most common frustration with tennis elbow, affecting 8 to 15 percent of patients. The three primary reasons for recurrence are: (1) stopping rehabilitation too early — before full tendon remodeling is complete, (2) returning to the same aggravating activities without ergonomic modifications, and (3) inadequate long-term maintenance exercise. A minimum of 4 weeks of continued exercise beyond pain resolution, combined with ongoing twice-weekly forearm stretches and strengthening, significantly reduces recurrence risk.
Does heat or ice work better for tennis elbow?
Both have roles at different stages. During the first 1 to 2 weeks (acute phase), ice is more appropriate — apply for 15 to 20 minutes after aggravating activities to manage acute pain. After the initial acute phase, heat applied before exercise sessions increases blood flow and tissue extensibility, improving the effectiveness of stretching and loading exercises. Many clinicians recommend a contrast protocol (alternating heat and ice) during the transition period.
How do I know if my tennis elbow is getting better?
Track these objective markers: (1) decreasing pain at rest, (2) increasing pain-free grip strength (measure with a hand dynamometer or simply note how heavy an object you can hold comfortably), (3) reduced morning stiffness duration, (4) ability to perform previously painful tasks with less discomfort, and (5) faster recovery after provocative activities. Pain during activity may fluctuate week to week, but these underlying metrics should show a positive trend over 4 to 8-week intervals.
Is it safe to lift weights with tennis elbow?
Lower body exercises (squats, deadlifts, leg press) are generally safe and encouraged to maintain overall fitness. For upper body work, avoid exercises that heavily load the wrist extensors — barbell rows, pull-ups, and bicep curls are common aggravators. Modify gripping exercises by using wrist straps to bypass the forearm extensors. As tennis elbow improves, gradually reintroduce gripping exercises at lighter weights, starting at 50 percent of your pre-injury loads.
What is the role of anti-inflammatory medication in tennis elbow recovery?
NSAIDs (ibuprofen, naproxen) can manage pain during the acute phase (first 1-2 weeks), but prolonged use beyond two weeks is not recommended. Research from the British Journal of Sports Medicine shows that chronic NSAID use may impair tendon healing by disrupting the inflammatory cascade that initiates repair. Use NSAIDs for short-term symptom management, not as ongoing treatment. Acetaminophen (paracetamol) provides pain relief without anti-inflammatory effects and may be preferable for longer-term use.
About the Author
Dr. Mark Stevens is a board-certified sports medicine specialist with over 15 years of clinical experience treating upper extremity tendinopathies. He completed his sports medicine fellowship at a major academic medical center and has published peer-reviewed research on tendon rehabilitation and regenerative injection therapies. Dr. Stevens treats recreational and competitive athletes as well as occupational injury patients, specializing in evidence-based conservative management of lateral and medial epicondylitis.
Sources and Methodology
This article synthesizes evidence from peer-reviewed clinical trials, systematic reviews, and established clinical practice guidelines. All treatment recommendations are graded by level of evidence. Product recommendations are independently selected based on clinical utility and are not influenced by affiliate relationships.
-
Coombes, B. K., Bisset, L., & Vicenzino, B. (2015). Management of Lateral Elbow Tendinopathy: One Size Does Not Fit All. Journal of Orthopaedic and Sports Physical Therapy, 45(11), 938-949.
-
Bisset, L., Beller, E., Jull, G., Brooks, P., Darnell, R., & Vicenzino, B. (2006). Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ, 333(7575), 939.
-
Smidt, N., van der Windt, D. A., Assendelft, W. J., et al. (2002). Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial. The Lancet, 359(9307), 657-662.
-
Peerbooms, J. C., Sluimer, J., Bruijn, D. J., & Gosens, T. (2010). Positive effect of an autologous platelet concentrate in lateral epicondylitis in a double-blind randomized controlled trial. American Journal of Sports Medicine, 38(2), 255-262.
-
Tyler, T. F., Thomas, G. C., Nicholas, S. J., & McHugh, M. P. (2010). Addition of isolated wrist extensor eccentric exercise to standard treatment for chronic lateral epicondylosis. Journal of Shoulder and Elbow Surgery, 19(6), 917-922.
-
Shaw, K. A., Dougherty, J. J., Treffer, K. D., & Glaros, A. G. (2015). Establishing the content validity and reliability of Patient-Rated Tennis Elbow Evaluation Questionnaire. Journal of Hand Therapy, 28(1), 19-26.
-
Weber, C., & Thai, V. (2019). Tendinopathy and tendon repair: Tendon structure, mechanobiology, and the role of exercise. British Medical Bulletin, 131(1), 67-79.
-
Stasinopoulos, D., & Johnson, M. I. (2005). Effectiveness of extracorporeal shock wave therapy for tennis elbow (lateral epicondylitis). British Journal of Sports Medicine, 39(3), 132-136.
-
Shaw, G., Lee-Barthel, A., Ross, M. L., Wang, B., & Baar, K. (2017). Vitamin C-enriched gelatin supplementation before intermittent activity augments collagen synthesis. American Journal of Clinical Nutrition, 105(1), 136-143.
-
American Academy of Orthopaedic Surgeons. (2024). Tennis Elbow (Lateral Epicondylitis): Clinical Practice Guidelines.
-
Vicenzino, B., de Vos, R. J., Alfredson, H., et al. (2020). ICON 2019 — International Scientific Tendinopathy Symposium Consensus. British Journal of Sports Medicine, 54(16), 941-954.
-
Shiri, R., Viikari-Juntura, E., Varonen, H., & Heliovaara, M. (2006). Prevalence and determinants of lateral and medial epicondylitis. American Journal of Epidemiology, 164(11), 1065-1074.
---
Walking Pad vs Treadmill
30-second comparison